Dangerous Coronary Blockages: Which Type of Blockage Is Most Risky for the Heart Attack?





Dangerous Coronary Blockages: Understanding the different types of heart blockages that lead to heart attacks can be lifesaving knowledge for patients and their families. While many people believe that the largest blockage is always the most dangerous, medical research reveals a far more complex picture. The type of blockage that causes a heart attack depends on various factors including location, composition, and stability of the arterial obstruction. This comprehensive guide will help you understand which blockages pose the greatest threat and why early detection matters.
🚨 Most Lethal Statistics:
💡 Eye-Opening Medical Facts:
🔍 Surprising Blockage Insights:

Coronary artery anatomy
The human heart receives blood through three main coronary arteries, each serving different regions of the heart muscle. When these arteries become blocked, the consequences vary dramatically based on which vessel is affected and how quickly the blockage develops.
Primary Coronary Vessels and Their Danger Levels:
Read Research Paper:
Complete blockage of a major coronary artery represents the most immediately life-threatening scenario. Unlike gradual narrowing that develops over years, acute occlusion occurs when:
According to recent clinical trials, patients experiencing complete acute occlusion have less than 90 minutes before irreversible heart muscle damage begins.
The statistics of widow maker blockages reveal why cardiologists consider this the most feared obstruction. This blockage affects:
Critical Supply Area: 60-70% of left ventricle blood supply Survival Rates: Only 50% survive if blockage is complete Time Factor: Death can occur within 15-30 minutes Detection Challenges: Often shows minimal symptoms before major event
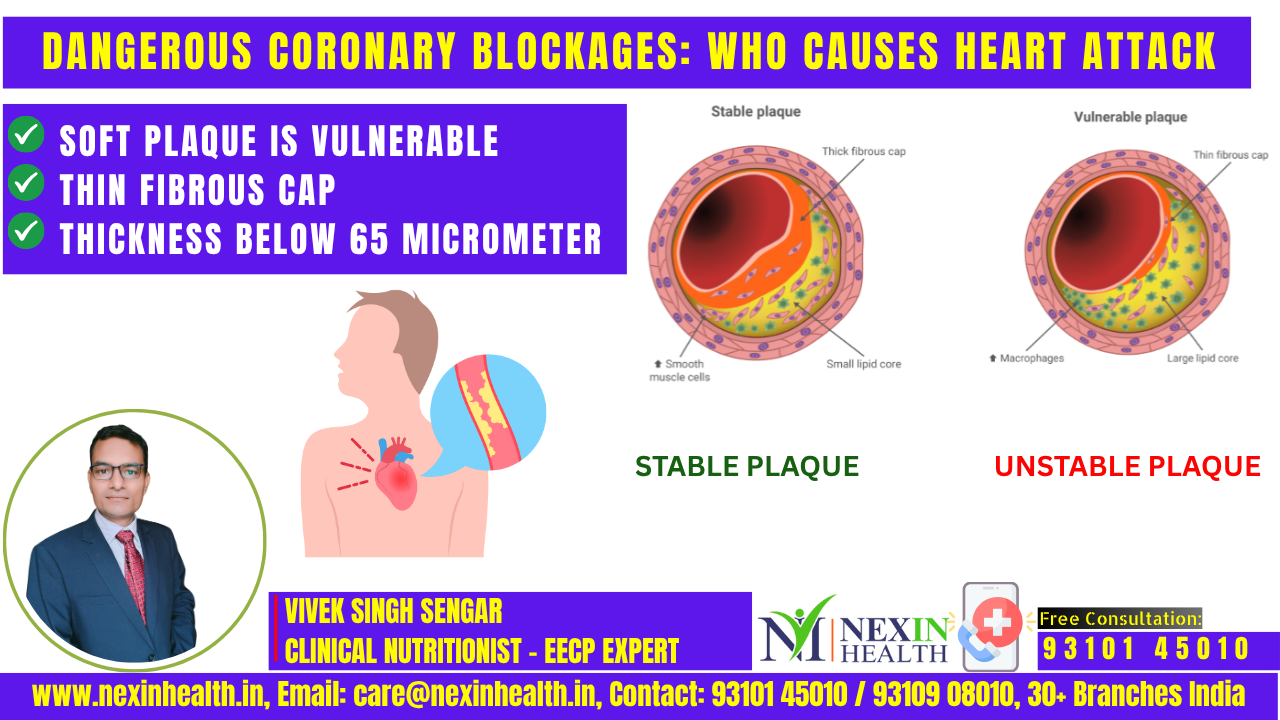
Paradoxically, some of the most dangerous blockages for heart attack are not the largest ones. Unstable plaques, often measuring only 40-60% blockage, cause the majority of heart attacks because:
Thin Fibrous Cap: Easily ruptures under stress Large Lipid Core: Forms massive clots when exposed Inflammatory Activity: Makes plaque highly unstable Unpredictable Timing: Can rupture without warning
The conventional approach to assessing blockage danger focused primarily on percentage of narrowing. However, modern cardiology recognizes that blockage composition and location matter more than size alone.
Stable vs. Unstable Blockages:
Stable blockages develop slowly over decades, allowing the heart to develop alternative blood pathways (collateral circulation). These gradually narrowing arteries may reach 80-90% blockage before causing symptoms.
Unstable blockages contain soft, cholesterol-rich material covered by a thin layer. These “vulnerable plaques” can rupture suddenly, causing immediate complete blockage through clot formation.
Blockages occurring in the first portion (proximal) of major arteries cause the most extensive heart damage because they cut off blood supply to the largest areas of heart muscle.
Benefits of Understanding Proximal Risk:
Mid-vessel blockages affect smaller portions of heart muscle but can still cause significant damage, especially in patients without adequate collateral circulation.
Blockages in the smaller, distant portions of coronary arteries typically cause less immediate danger but can still result in heart attacks in vulnerable patients.
Certain conditions make any type of blockage significantly more dangerous:
Diabetes: Causes multiple small vessel disease and silent blockages High Blood Pressure: Increases plaque rupture risk Smoking: Makes blood more likely to clot Family History: Genetic factors affecting plaque stability
Age: Reduced ability to develop collateral circulation
Modern lifestyle patterns common in urban areas contribute to dangerous blockage formation:
Traditional symptoms that indicate dangerous blockage causing heart attack:
Women, diabetics, and elderly patients often experience different symptoms:
When dealing with dangerous blockages causing heart attack, time equals heart muscle. The “golden hour” concept emphasizes:
First 30 Minutes: Call emergency services immediately 30-90 Minutes: Emergency room evaluation and treatment initiation 90 Minutes-6 Hours: Optimal window for emergency procedures Beyond 6 Hours: Significant permanent heart damage likely
Emergency Angioplasty: Best option for complete acute blockages Clot-Dissolving Medications: Effective for certain types of blockages Emergency Bypass Surgery: Reserved for complex multi-vessel blockages Medical Management: For stable blockages with ongoing monitoring
Medication Management:
Lifestyle Modifications:
Modern cardiac testing can identify dangerous blockages before they cause heart attacks:
Coronary Angiography: Gold standard for detecting blockages CT Coronary Angiogram: Non-invasive blockage detection Stress Testing: Identifies functionally significant blockages Calcium Scoring: Detects early arterial changes
Patients who survive dangerous blockages require lifelong management:
Cardiac rehabilitation programs specifically designed for blockage survivors include:
1. Which type of blockage is most dangerous for heart attack?
The most dangerous blockage is complete acute occlusion of the left main coronary artery or proximal left anterior descending artery (widow maker). These blockages can cause death within 15-30 minutes and affect 60-75% of the heart muscle.
2. Can a small blockage cause a fatal heart attack?
Yes, unstable plaques with only 40-50% blockage cause 70% of heart attacks. These soft, cholesterol-rich blockages can rupture suddenly and form large clots that completely block the artery.
3. How quickly can a dangerous blockage kill you?
Complete blockage of the left main coronary artery can cause death within 15-30 minutes. The widow maker blockage has a 50% fatality rate, with many deaths occurring before reaching the hospital.
4. What makes one blockage more dangerous than another?
Location matters more than size. Blockages in proximal portions of major arteries are most dangerous because they cut off blood supply to larger areas of heart muscle. Unstable plaque composition also increases danger significantly.
5. Are there warning signs before a dangerous blockage causes heart attack? Some patients experience warning symptoms like unusual fatigue, chest discomfort with exertion, or shortness of breath. However, 50% of heart attacks occur without any prior symptoms, especially with unstable plaque rupture.
6. How do doctors determine if a blockage is dangerous?
Doctors use angiography, stress tests, and advanced imaging to assess blockage location, size, and stability. They also consider patient factors like diabetes, age, and collateral circulation development.
7. Can dangerous blockages be treated without surgery?
Treatment depends on blockage type and timing. Emergency angioplasty is preferred for acute complete blockages. Some stable blockages can be managed with medications, while others require surgical bypass.
8. Do dangerous blockages always cause chest pain?
No, especially in women, diabetics, and elderly patients. Dangerous blockages can cause atypical symptoms like jaw pain, back pain, nausea, or just unusual fatigue. Silent heart attacks are common in diabetic patients.
9. How long do you have to get treatment for a dangerous blockage?
The optimal treatment window is within 90 minutes of symptom onset. However, treatment can be beneficial up to 12 hours after heart attack begins, though heart muscle damage increases with time.
10. Can you prevent dangerous blockages from forming?
Yes, through comprehensive prevention including cholesterol management, blood pressure control, diabetes management, regular exercise, healthy diet, stress reduction, and smoking cessation. Regular cardiac screening helps detect dangerous blockages early.
11. What’s the survival rate for different types of dangerous blockages?
Survival rates vary: Left main blockage (50% survival), Widow maker (60-70% survival with prompt treatment), Right coronary artery complete blockage (80-85% survival), and unstable plaque rupture (90-95% survival with emergency treatment).
12. How do you know if you’re having a heart attack from a dangerous blockage?
Call emergency services immediately if you experience crushing chest pain lasting over 15 minutes, especially with sweating, nausea, shortness of breath, or pain radiating to arm, jaw, or back. Don’t wait – dangerous blockages require immediate medical attention.
Also Read:
EECP Treatment for Heart Failure
Track Heart Failure with 6 Minute Walk Test
_____________________________________________________________________________
Mr. Vivek Singh Sengar is the Founder of Fit My Heart and a leading Integrated Health Practitioner & Clinical Nutritionist at NEXIN HEALTH and MD City Hospital Noida. With over 13 years of experience, Vivek has treated more than 25,000 patients suffering from lifestyle diseases like heart disease, diabetes, and obesity through non-invasive, drugless, and nutrition-focused therapies.
His expertise combines modern medical knowledge with traditional Indian healing practices to provide comprehensive care for heart failure patients. Vivek’s approach focuses on sustainable lifestyle modifications, nutritional therapy, and patient education to achieve optimal cardiovascular health outcomes.
Get Expert Guidance for Your Heart Health:
📧 Email: care@nexinhealth.in
📞 Phone: +91 93101 45010
💬 WhatsApp: Click to Chat
Take the first step towards better heart health today. Contact our team for personalized heart failure management plans tailored to your specific needs and lifestyle.


Experience

Certified Therapists

Satisfied Patients
Contact us